Osteopathy for Babies – KISS Syndrome
Screaming Babies, Sleep Problems, Head Tilting – What Now?
The term KISS Syndrome can be heard more and more often when talking about children who cry a lot, only turn their head to one side, overstretch, and don’t sleep through the night. Frequently there are also problems with breastfeeding and digestion. So-called KISS children display concentration problems and hyperactivity when they are of kindergarten or school age.
Opinions held by conventional medical practitioners regarding the KISS Syndrome diverge heavily in parts from those held by representatives of osteopathy.
The camp of mainstream physicians does not have a uniform standpoint. Dr. med. H. Biedermann established the term KISS (Kinematic Imbalance due to Suboccipital Strain) for children with the symptoms described above.
Prof. Dr. med. R. Stücker, head physician of the Children’s Hospital Altona and one of the leading pediatric orthopedists in Northern Germany has a different viewpoint. He questions the existence of such a diagnosis.
Different authors using varying terms synonymously at times has lead to inconsistent terminology. Some authors use the term torticollis or “nursing infant asymmetry.” Terms like “wryneck”, “stiff neck”, “cervical dystonia”, “head tilt”, “caput obstipum”, and “twisted neck”, “crooked neck” as well as “colum distortum” also appear in the nomenclature; these are partly used as synonyms for “torticullis” and “muscular wryneck”.

Authors writing about osteopathy only rarely use the term KISS Syndrome. Whether one decides to use this actual term or not – children with the above described symptoms do present at osteopathic clinics. It is more important to the osteopath to treat the child than to worry about inconsistent terminology.
The cause for the development of a KISS Syndrome or rather, of symptoms that occur in connection with this term, can often be found already at birth, where the child is subjected to massive forces.
The literature names wryneck, face and skull asymmetry, fixed lateral positions of neck and torso, asymmetry of the buttocks folds, asymmetrical use of arms and legs as well as delayed maturing of joints on the inner side of where the body bends, and a flattening of the skull on one side as the most important symptoms for “KISS”.
A fixed arching back of the head, especially when sleeping and an asymmetrical flattening of the back of the head can be observed. In addition, the following can occur: overstretching, shoulder raising, arms in a handle or plane position, bad support when lying on the tummy, weak mouth and head posture muscles, breastfeeding problems on one side, and cold and/or sweaty hands (Biedermann 2007; Sacher 2007).
“KISS theory” places all the blame for the described symptoms on a blockade of the head joints.
At our osteopathic clinic we would like to open people’s eyes to the fact that there might be other causes involved as well:
When one considers the numerous connections of the head joints to other body structures, it makes sense that the head joints might be influenced by problems or tensions in one of the described structures by way of said connection.
This presupposes that it is possible to have an influence on said connections. This is obvious to all therapists practicing osteopathy. Those adhering to conventional medicine might agree to the extent that they acknowledge this concept and attribute significance to the fasciae connections.

Anatomically the cranial joints are described as a hinged connection between the atlas (1st cervical vertebra) and occipital bone (upper cranial joint; Art. atlantooccipitalis) as well as between atlas and axis (lower cranial joint; Art. atlantoaxiales) (Schünke et al. 2009; Benninghoff et al. 2008).
The dura mater (cerebral membrane) (illustr.) starts at the inside of the skull bone, at the top and below of the atlas vertebra and at the same height as the iliosacral joints (Wildgruber 2012). It attaches to the crista galli, crista frontalis, sulcus sinus sagitalis ossis frontalis, sulcus sinus sagitalis ossis occipitalis, sinus rectus and confluens sinuum, sulcus sinus transversus ossis ossipitalis, angulus mastoideus ossis parietalis, sulcus sinus petrosus ossis superiores, processus clinoideus anterior and posterior, and at the foramen magnum (all areas of skull bones), C2/C3 (cervical spine), at the sacrum (sacral bone) and at the coccyx (tailbone) (Paoletti 2011; Liem 2009). We can therefore see that there is a continuity between the skull joints and the pelvis, in addition to the bony connection via the spinal column.
The galea aponeurotica (tendon hood) starts at the back of the head at the external occipital protuberance and forms a connection to the temporal, parietal, and frontal bones (skull bones). It continues via the fascia temporalis into the fascia masseterica, on to the fascia cervicalis superficialis. There is also a connection to the skin and to the dura mater (cerebral membrane).
The fascia temporalis has a continuity to the other face fasciae and therefore to the zygoma, maxilla (skull bone), and to the ductus parotideus (parotid duct). The face fasciae cover the fascia cervicalis superficialis and surround the muscles of mastication.
Die fascia cervicalis superficialis surrounds the neck with the sternocleidomastoid and trapezius muscles as well as the neck muscles and the tongue bone (hyoid). In the area of the hyoid it connects to the middle neck fascia, the fascia cervicalis medialis, and continues into the fascia endothoracica and the other fasciae of the torso.
The fascia cervicalis media surrounds the infrahyoid musculature and the scalene muscles and, together with the fascia cervicalis profunda, forms the fascia prevertibralis which lies in front of the vertebrae.
In a cranial direction, the fascia cervicalis medialis has a continuity, inter alia, to the occiput and therefore to the cranial joints and through its deep layers forms a sheath for the larynx (voice box), thyroid and parathyroid gland, trachea (windpipe), pharynx (throat), and esophagus (gullet).
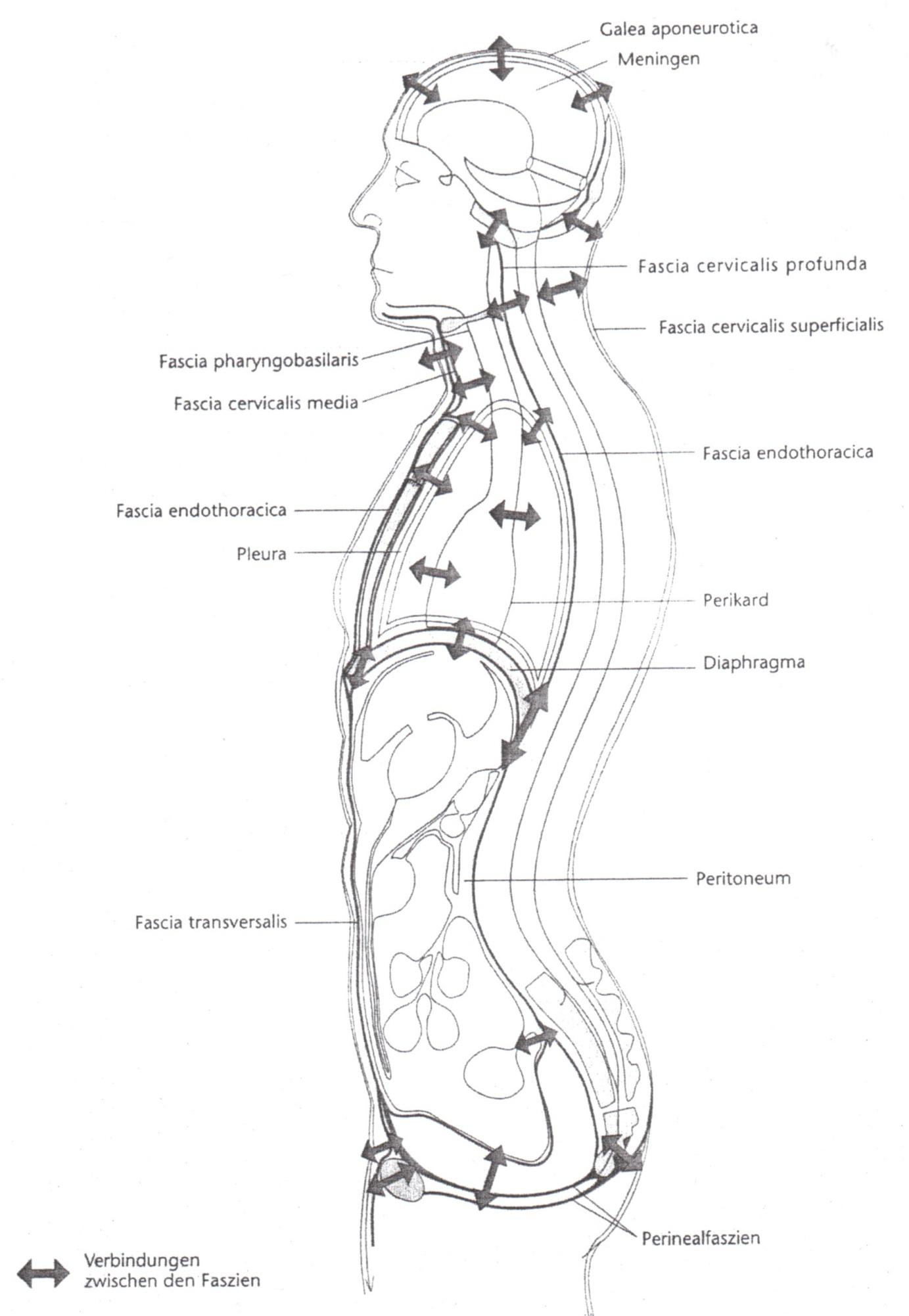
In addition, there are the following bony insertion points: sternum (breastbone), clavicle (collarbone), and the first ribs.
The fascia cervicalis profunda or prevertebralis comes cranially from the pars occipitalis of the base of the skull and is anterior (in front) of the spine; it surrounds the paraspinal and prevertebral musculature, the plexus cervicalis, plexus brachialis, the truncus sympathicus, as well as the phrenic nerve, the vertebral artery and the vertebral vein. Like the fascia cervicalis media, it leads into the fascia endothoracica.
The fascia endothoracica lines the inside of the thoracic cavity and has a connection with the ribs. It covers the diaphragm and continues through it by way of the fascia transversalis to the abdominal wall. It thickens cranially and forms the cervicothoracic diaphragm, where the pleura is suspended above the suspensory ligament . Thus there is a connection to the lungs, the diaphragm, and the pericardium.
The fascia transversalis lines the inside of the abdomen and has a connection to the organs in the lesser pelvis. It continues in the abdominal fasciae (stomach fascia), in the peritoneum, the fasciae of the lower extremities, and the fascia renalis (kidney fasciae). Through this connection there is a continuity – in the broadest sense – between the cranial joints and the abdominal organs as well as the pelvis and the lower extremities (Paoletti 2011).
The gastrointestinal tract is suspended from the base of the skull by the esophagus (gullet) (Helsmoortel 2002). The most important fixed points here are the pharyngeal tubercle of the occiput and the pterygoid processes of the sphenoid bone (Paoletti 2011).
Dysfunctions in the area of the visceral system can represent a disruptive factor for the functionality of the cranium through the described connection of the base of the skull and therefore also the cranial joints with the gastrointestinal tract.
From an osteopathic viewpoint, what are the consequences of impairment of the cranial joints?
Blockages that developed in the craniosacral system, for example at birth, lead to heighten tensions of the dura mater, which leads to overstretching through the asymmetrical blockage and presents symptoms like cranial asymmetry, wryneck, and pelvic obliquity (Wildgruber 2012).
Nerves or their microscopic supply vessels can be negatively affected by abnormal stresses or tensions in the soft tissue or cartilage structures of the base of the skull (Carreiro 2004).
An irritation of the head joints or tensions between the occipital and temporal bones lead to a narrowing of the jugular foramen and therefore to an impairment of the structures that emerge here. The following run through the jugular foramen: the jugular vein, as well as the cranial nerves 9 (glossopharyngeal nerve), 10 (vagus nerve) and 11 (accessory nerve).
Through tensions of the connective tissue, the muscles, or the cartilage components, the sensitive structures running through the jugular foramen as well as the hypoglossal nerve (12th cranial nerve), which runs through the hypoglossal canal can become irritated (Opalka 2008; Wildgruber 2012; Carreiro 2004).
Problems with sucking and swallowing can be the result of an irritated glossopharyngeal nerve.
Vegetative problems with hypertension of the gastrointestinal tract and therefore the functional symptoms of nursing infants like hiccups, vomiting, severe burping, problems with bowel motions, and wind, can be the result of an impeded vagus nerve (Opalka 2008; Wildgruber 2012; Carreiro 2004). “Clinically the vagus nerve is negatively affected by lesions of the cervical vertebra, tongue bone, upper thoracic vertebrae, and upper ribs as well as the muscle contractions in these regions and peripherally through foreign objects or diseases of the mucous membrane, which lines the various cavities irritated by the vagus nerve.” (Clark 2005).
If the accessory nerve is irritated, it leads to muscular disorders and can cause torticollis (wryneck), because it can result in a tonus change of the sternocleidomastoid and the trapezius muscles (Clark 2005; Opalka 2008; Bloß 2013).
The most frequent disorder of the hypoglossal nerve is in the form of motoric effects on the tongue, in connection with problems swallowing and chewing. (Clark 2005).
It is highly probably that a tight skull base goes hand in hand with the symptom complex of crying, irritability, and colics. What is meant by this is an increased density in the area of the skull base. However, it must be emphasized that bowel motility and function of a nursing infant is still immature at first and therefore the tight base of the skull cannot be made solely responsible for colics (Carreiro 2004).
The shoulders and clavicles (collarbones) can also affect the hyoid (tongue bone) via the omohyoid and sternohyoid muscles. According to Carreiro (2004) biomechanical stresses in each of these structures can impede the effectiveness of sucking.
According to Clark (2005) all cranial nerves are affected by lesions of the cervical and upper thoracic vertebrae.
Dysfunctions in the area of the visceral systems (organ system) will present a source of irritation for the functionality of the cranium through the fascial connections of the base of the skull and therefore also through the connections of the cranial joints with the gastrointestinal tract. Via this connection the visceral system can transfer mechanical information to the occiput and sphenoid (Guerrassimiouk 2003).
Experience has shown that treating the affected structures with osteopathic techniques usually leads to a marked improvement of the symptoms.
Bibliography KiSS Syndrome and Osteopathy:
Benninghoff; D. (2008): Taschenbuch Anatomie. 1st Edition Munich: Urban & Fischer .
Biedermann, H. (2007): KISS-Kinder. 3rd Edition Stuttgart: Thieme Verlag.
Bloß, C. (2013): Die funktionelle Säuglingsasymmetrie- Welche Risikofaktoren spielen eine wichtige Rolle und in welchem Zusammenhang stehen die Anpassungsstörungen?. 1st Edition Saarbrücken: AV Akademikerverlag .
Carreiro, J. E. (2004): Pädiatrie aus osteopathischer Sicht: Anatomie, Physiologie und Krankheitsbilder. 1st Edition Munich: Urban & Fischer .
Clark, M. E. (2005): Angewandte Anatomie. 1st German Edition: Édition Spirales .
Guerrassimiouk, D. (2012): „Die physiologische Entwicklung in den ersten Lebensjahren“. DO- Deutsche Zeitschrift für Osteopathie [German Journal of Osteopathy], 2012, No. 4, pp. 23-27.
Helsmoortel, J. (2002): Lehrbuch der visceralen Osteopathie. Stuttgart, New York: Georg Thieme .
Liem, T. (2009): Kraniosacrale Osteopathie: Ein praktisches Lehrbuch. 5th Edition: Hippokrates.
Opalka, M (2008): „Das KiSS-Syndrom: nicht existent oder tägliches Brot?“. DHZ – German Naturopathic Magazine, 2008, No. 3, pp. 34 – 37
.
Paoletti, S. (2011): Faszien- Anatomie, Strukturen, Techniken, Spezielle Osteopathie. 2nd Edition: Urban & Fischer.
Sacher, R. (Juni 2007): Handbuch KISS KIDDs: Entwicklungsauffälligkeiten im Säuglings-/Kleinkindalter und bei Vorschul-/Schulkindern – Ein manualmedizinischer Behandlungsansatz, 3rd Edition Dordmund: Verlag modernes lernen.
Schünke, M.; Schulte, E.; Schumacher, U.; Voll, M.; Wesker, K. (2009): Prometheus- Kopf, Hals und Neuroanatomie. 2nd Edition Stuttgart: Thieme.
Wildgruber, H. (2012): „Geburtstraumatisch bedingte Blockierungen an Schädel, Wirbelsäule und Becken des Säuglings“. OM- Osteopathic Medicine, 13th Vol., Issue 2/2012, pp. 9-11, Elsevier GmbH- Urban & Fischer.
